
Do you suffer anterior knee pain? Part 1 of 3.

Pain below, under or around the knee cap is common in people who do activities which place increased load on the quads.
?Pain is often exacerbated with stairs, running and plyometric (explosive) activities. Pain may reduce with exercise initially (warm-up phenomenon) but come back worse the day after activity.
⏰Tendon injuries take time to heal due to limited blood supply and changes in collagen formation.
?Tendons love load so in order to minimise pain we must progressively increase load tolerance. Loading in a pain range of 3-4 out of 10 and progressing exercises adequately depending on each individual case.
?The whole lower limb kinetic chain must be assessed for key biomechanical factors that may play a role in the development of anterior knee pain.
Without addressing these factors, increasing load tolerance of the quad tendon may not be enough to fix anterior knee pain.
Exercises for anterior knee pain. Part 2 of 3.
1️⃣ LEVEL 1 |
Extend the knee against the resistance of a light band. Repetitive concentric quad contraction with isometric holds allows initial adaptation to occur at the quad tendon without overloading and re-injury.
Pain during and after this exercise should remain below 4/10.
2️⃣ LEVEL 2 |
Single leg step-downs – Start with a lower step height and low weight (can hold wall to support body weight) and work up to a higher height with additional weight.
Spanish squats – Maintain a vertical tibia/shin angle to recruit max quad contraction, whilst placing eccentric load across the tendon. Work within a pain level of 4/10. If pain following exercise is worse, reduce the load and/or reps to allow the body to adapt.
3️⃣ LEVEL 3 |
Single leg control – Perform a single leg squat to a chair, maintain stable knee position. Progress to deeper squat and higher reps. Landing mechanics – The ability to appropriately attenuate force through tendons muscles and joints is vital before return to running and plyometrics. With decreased control in landing techniques being associated with higher incidences of tendon injuries. Plyometrics – To be introduced once landing mechanics have been perfected. This is to adequately reintroduce the storage and conversion of energy in the tendon.
Exercises for anterior knee pain. Part 2 of 3.1️⃣ LEVEL 1 |Extend the knee against the resistance of a light band. Repetitive concentric quad contraction with isometric holds allows initial adaptation to occur at the quad tendon without overloading and re-injury. Pain during and after this exercise should remain below 4/10.2️⃣ LEVEL 2 |Single leg step-downs – Start with a lower step height and low weight (can hold wall to support body weight) and work up to a higher height with additional weight. Spanish squats – Maintain a vertical tibia/shin angle to recruit max quad contraction, whilst placing eccentric load across the tendon. Work within a pain level of 4/10. If pain following exercise is worse, reduce the load and/or reps to allow the body to adapt.3️⃣ LEVEL 3 |Single leg control – Perform a single leg squat to a chair, maintain stable knee position. Progress to deeper squat and higher reps. Landing mechanics – The ability to appropriately attenuate force through tendons muscles and joints is vital before return to running and plyometrics. With decreased control in landing techniques being associated with higher incidences of tendon injuries. Plyometrics – To be introduced once landing mechanics have been perfected. This is to adequately reintroduce the storage and conversion of energy in the tendon
Posted by Trident Movement on Tuesday, June 18, 2019
Biomechanical Considerations for anterior knee pain. Part 3 of 3
Deficits in lower limb biomechanics such as atypical joint range of motion or weakness in antigravity muscles can lead to the development of anterior knee pain as a secondary injury.
Unfortunately, it’s not always that simple. Other risk factors such as weight, prior injury, training regime, behavioural and psychological habits can also play a role.
1️⃣ HIP FLEXION |
Limited hip flexion leads to excessive knee flexion and therefore increased force across the patellofemoral joint. Assessing for asymmetry in hip flexion right to left, which correlates with pain, may be important.
2️⃣ ANKLE DORSIFLEXION |
Limited ankle dorsiflexion affects knee biomechanics and asymmetry can be associated with higher incidences of knee pain.
3️⃣ POOR SINGLE LEG CONTROL |
Asymmetry in leg range of motion and/or muscle control can lead to an imbalance of load placed on the knee and patellofemoral joint.
Biomechanical considerations for anterior knee pain. Part 3 of 3.Deficits in lower limb biomechanics such as atypical joint range of motion or weakness in antigravity muscles can lead to the development of anterior knee pain as a secondary injury..Unfortunately, it’s not always that simple. Other risk factors such as weight, prior injury, training regime, behavioural and psychological habits can also play a role.1️⃣ HIP FLEXION | Limited hip flexion leads to excessive knee flexion and therefore increased force across the patellofemoral joint. Assessing for asymmetry in hip flexion right to left, which correlates with pain, may be important..2️⃣ ANKLE DORSIFLEXION | Limited ankle dorsiflexion affects knee biomechanics and asymmetry can be associated with higher incidences of knee pain..�3️⃣ POOR SINGLE LEG CONTROL | Asymmetry in leg range of motion and/or muscle control can lead to an imbalance of load placed on the knee and patellofemoral joint….#kneepain
Posted by Trident Movement on Wednesday, June 19, 2019
➡️POTENTIAL PATHWAYS of patellofemoral pain
Please note that these are examples of SOME exercises and progressions. Each case is unique and the rehabilitation process operates on a continuum whereby there should be a graded progression or regression based upon many factors. The complexity of patellofemoral pain and musculoskeletal pain should not be under estimated based upon some videos sen on social media.
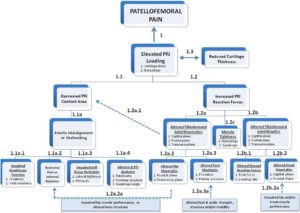
A schematic overview of potential pathways to anterior knee pain from Powers CM, et al. Br J Sports Med 2017
Pictured above is a schematic representing other factors associated with anterior knee pain that must be considered clinically.
